
Basic Chest X-RayInterpretation
Adam Guttentag, M.D.
© Copyright Adam Guttentag, MD
All Photos Retain the Copyrights of Their Original Authors
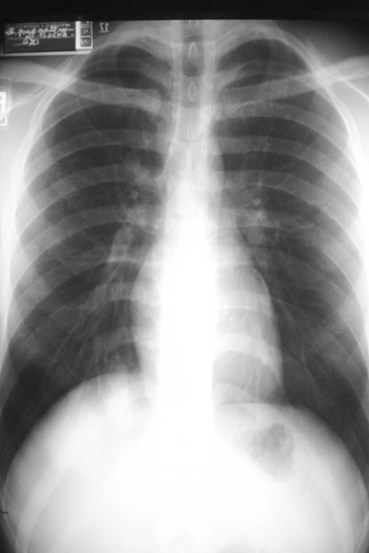
How do you look at achest x-ray?
Avoid tunnel vision!Avoid tunnel vision!
or





Chest wall, bones and abdomen



Mediastinum, heart and hila

Lungs
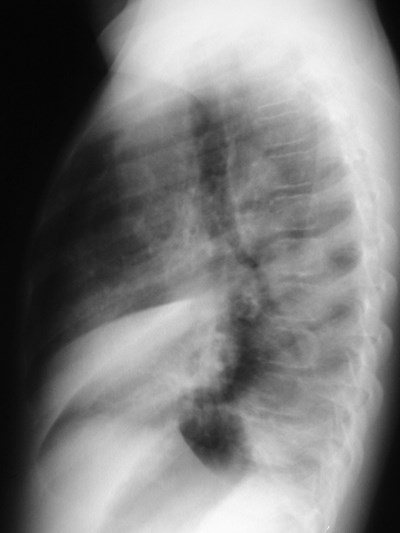
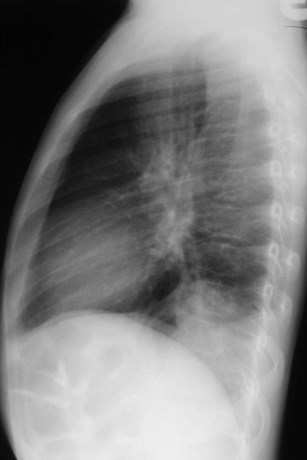
The Lateral Chest Film
•Find abnormalitieshidden on the frontalfilm
•Confirmabnormalitiessuspected fromfrontal film
•Don’t be afraid tolook at it!

Our best friend!
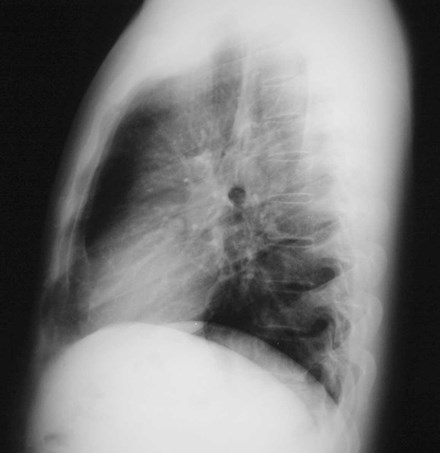
Looking at the lateral CXR


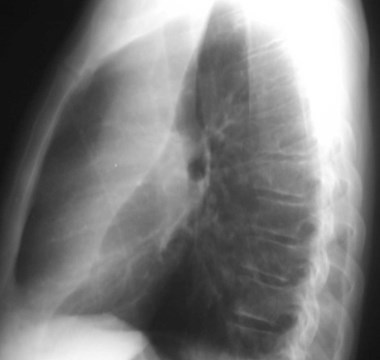
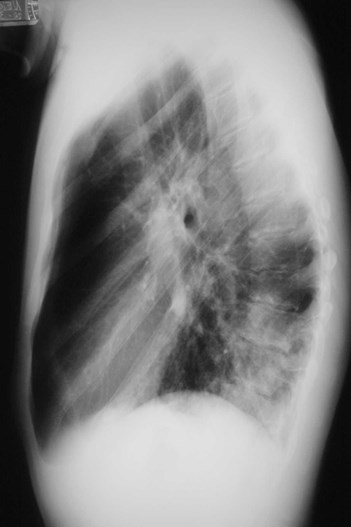
Hilar structures on the lateral film:



“Ring around thebronchus”
Technical Factors
•Positioning
straight vsoblique

(How we’ll try to fool you)


Effect of obliquity on heart size
Technical Factors
•Positioning
straightvs oblique
PA vs AP
Technical Factors
•Positioning
straight vsoblique
PA vs AP
erect vssupine


erect
supine
Technical Factors
•Positioning
straight vsoblique
PA vs AP
erect vs supine
lordotic vskyphotic




lordotic
kyphotic
Technical Factors
•Positioning
straight vsoblique
PA vs AP
erect vssupine
lordotic vskyphotic


Effect on mediastinal contour
Technical Factors
•Depth of inspiration
•Visualization ofpathology depends oncontrast provided by airin the lungs
•Count ribs!

10

8
Short of breath

One minutelater
8
Technical Factors
Body habitus

Radiographic technique:
Is it really different?
Changing technique can makedisease look better or worse.



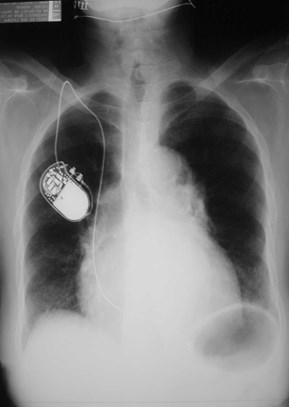
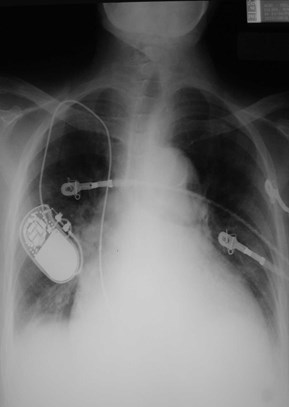
Is the heart large? Is themediastinum wide?
Same patient, 4 films within one month
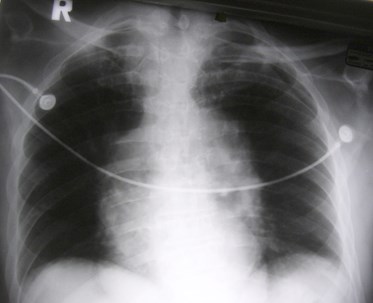
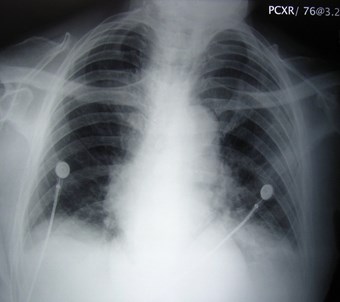
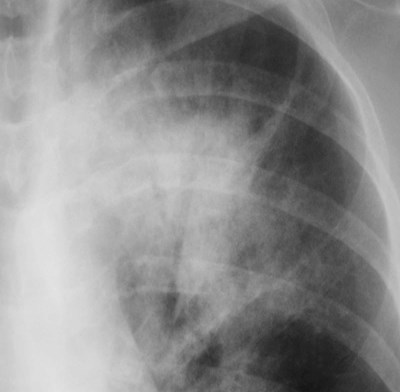
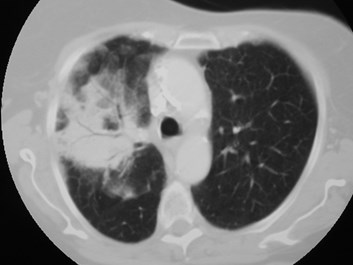
Recognizing air space disease
•Alveolar spaces filled with…something.
•Radiologists’s report:
“consolidation”
“air space opacity”
“fluffy density”
“infiltrate”
•Nonspecific:
Atelectasis, pneumonia, bleeding, edema, tumor
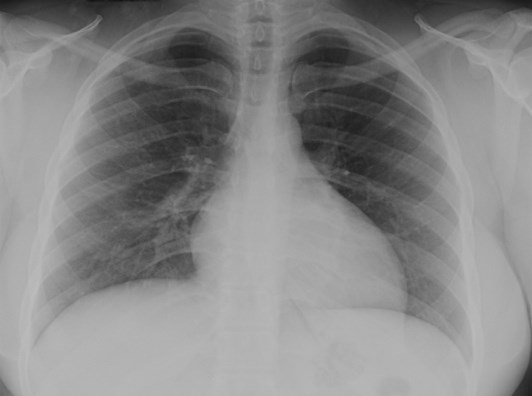
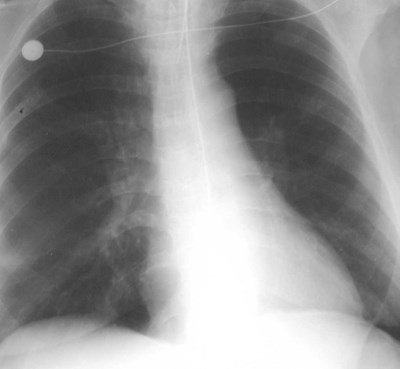
The Silhouette Sign
•Indicates air space disease.
•Obscuration of a normally seenborder, e.g. diaphragm or heart.
•Opacity with sharp edge along afissure.
Localizing disease from thesilhouette sign
RLL
RML
LLL
Lingula
LLL
Localizing disease from thesilhouette sign
RUL
RML
UL
LL
RML orlingula

16 hours later
What happened here?What happened here?
Lobar Atelectasis
•Best sign -- shift of a fissure
•Rapid development and clearance
•Air bronchograms if non-obstructive
•Secondary signs:
Mediastinal shift
Elevated diaphragm
Ribs closer together
Vague increased density


LLL Atx
Next day


RUL Atx

RML Atx

LUL Atx
Pneumonia
•Signs
Air bronchogram
Silhouette - “positive” or “negative”
Dense hilum
“Spine” sign
•All are signs of any air space process
•Dx of pneumonia depends on appropriateclinical scenario.
Air bronchogram sign
Pseudomonaspneumonia
Lung cancer
Air bronchograms—CT

Pneumonia
Lung cancer


Right middle lobe


Right upper lobe

Right lower lobe
Posterior diaphragm silhouetted


Dense hilum, spine sign


Dense hilum, spine sign again

Four days later
Final Exam

21 y.o. with fever and cough
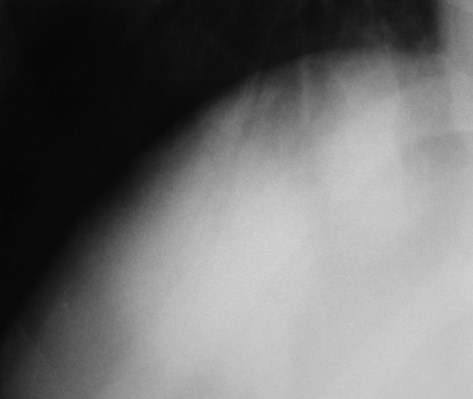

Hyperlucenthemithorax: why?

Did you notice the mass?
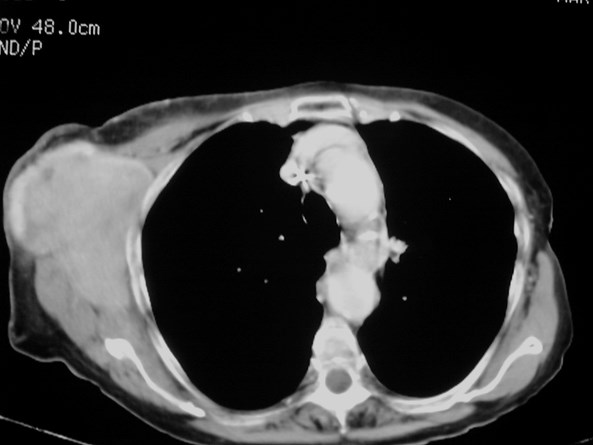
Lymphoma
Take home message #1
It’s a chest x-ray,
not a lung x-ray.

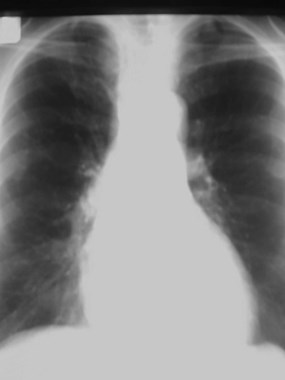

6 cm lung mass missed. How?
2 years ago
Take home message #2
Old films are your friend!

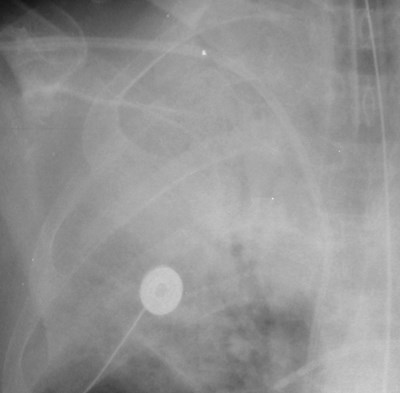
Elderly man with hypotension

Suddenly septic

Pneumatosis of small bowel
Take home message #3
The patient pays forthe whole film!
Questions
All are kinds of air spacedisease except
•Hemorrhage
•Pneumonia
•Tumor
•Sarcoidosis
•Atelectasis
The most specific sign ofatelectasis is:
•Obscuration of a diaphragm
•Shift of a fissure
•Air bronchograms
•Density over the spine
•Mediastinal shift
This can make the heart looklarger than it is:
•Lordotic positioning
•AP positioning
•Expiratory film
•Supine positioning
•All of the above
Reading